ARTICLE
HOW HYALURONIC ACID EXPANDS THE RANGE OF APPLICATIONS FOR ALLOGENEIC BONE MATERIAL
Regenerative concepts that are not only biologically convincing but also facilitate surgical handling are particularly sought after in complex augmentation cases. An innovative approach is the combination of the allogeneic bone substitute maxgraft® with hyaluronic acid (HyA), a substance known in regenerative medicine for its cell-stimulating and wound-healing properties. The aim is to promote new bone formation while optimizing the moldability and application of the material.
One person who recognized the potential of this combination early on is oral and maxillofacial surgeon Prof. Dr. Dr. Eik Schiegnitz, head of the Department of Implantology at the University Medical Center Mainz, Germany. In an interview with specialist journalist and dentist Dr. Aneta Pecanov-Schröder, he describes his experiences with maxgraft® + HyA (botiss biomaterials, Straumann Group) in everyday clinical practice—from ridge preservation to complex vertical defects and sinus floor augmentations.
Professor Schiegnitz, maxgraft® has proven itself clinically for years thanks to its excellent biomechanical and osteoconductive properties.
This allogenic bone granulate is based on human donor bone, which is processed using Cells+ Technology and manufactured in Germany.
For almost two years, the material has also been available in combination with high-molecular hyaluronic acid (HyA), pre-portioned in glass containers and easy to activate immediately before use. The result is a gel-like, moldable consistency that is particularly easy to shape.
How long have you been using maxgraft® + HyA, and for which indications has this combination proven particularly successful in your clinic?
Prof. Schiegnitz: I have been working regularly with maxgraft® + HyA for about two years, mainly for immediate concepts, horizontal and vertical ridge defects, and more complex sinus floor augmentations. The combination has also proven very helpful in ridge preservation cases where immediate concepts are contraindicated.
The decisive advantage lies in improved clinical handling combined with biologically supported bone regeneration. The combination contributes significantly to overall harmonious tissue integration and improved treatment planning.
What role does the allogenic nature of the material play for you in comparison to autologous or xenogeneic alternatives, and what convinces you about the combination product from a surgical point of view?
Prof. Schiegnitz: From a surgical point of view, I am particularly impressed by the high cohesion and dimensional stability of the bone graft. Due to the combination with hyaluronic acid, maxgraft® granules transform into a gel-like, moldable mass, a kind of ‘sticky bone’, that can be precisely placed and adapted in the defect site. This is particularly advantageous for complex ridge defects or sinus lift procedures.
The viscoelastic properties enable precise modeling, and the shape is retained even under mechanical stress. This facilitates defect filling, ensures stable augmentation, and supports the use of membranes, for example, in smaller, limited defects. The material stays where it belongs without drifting easily or escaping from the defect.
Another practical advantage is that maxgraft® + HyA is ready for use immediately after mixing with saline solution. No additional materials, such as blood or NaCl, are required, which saves time and reduces variability in surgical preparation.
In my opinion, allogeneic materials offer an ideal compromise between biological regeneration and patient comfort. The fact that a second extraction site is not required means significantly lower morbidity. In addition, many patients show a clear preference for human materials over animal products.
What are the biological advantages of adding hyaluronic acid?
Prof. Schiegnitz: From a biological perspective, hyaluronic acid stimulates crucial processes in the early phase of healing. It has been proven to support cell migration and angiogenesis, promote the early migration and activation of osteoblasts, fibroblasts, and endothelial cells, and thus contributes significantly to the revitalization of the graft. HyA acts as a biological signal matrix that specifically improves the regenerative environment in the critical initial phase of bone healing.
These early processes are essential for stable and high-quality bone formation. In addition, hyaluronic acid is known for its anti-inflammatory effect, which can have a positive influence on early wound healing. Initial clinical observations indicate a favorable tissue response and reduced postoperative irritation.
These synergistic effects make maxgraft® + HyA a practical solution for modern augmentation concepts with clear advantages in both biological integration and surgical handling.
Although the individual components have been well studied, only limited clinical (long-term) studies on the combination of maxgraft® + HyA are available to date.
Prof. Schiegnitz: Initial practical reports however confirm good volume stability and healing. Animal models also show improved tissue integration and increased vascularization.
The first clinical study comparing allogeneic bone replacement materials with and without hyaluronic acid in the context of alveolar ridge preservation was conducted under the direction of maxillofacial surgeon Priv.-Doz. Dr. Dr. Frank Kloss [1] from Lienz, Austria. The results show that supplementation with hyaluronic acid in compromised extraction sockets leads to significantly better clinical outcomes. These include higher graft stability, lower resorption rates, and increased bone mineral density.
A study by Nistor et al. [2] also suggests that hyaluronic acid as a biological additive has the potential to positively influence both bone regeneration and soft tissue healing.
However, robust clinical data and standardized protocols will be necessary in the future to make informed, evidence-based decisions. The results to date are promising, and the scientific evidence on the benefits and synergistic effects of this combination is growing steadily.
You use maxgraft® + HyA in particular for immediate concepts, horizontal and vertical ridge defects, in selected cases of ridge preservation, and for more complex sinus floor augmentations. Could you please illustrate your approach using a case study from immediate implantation?
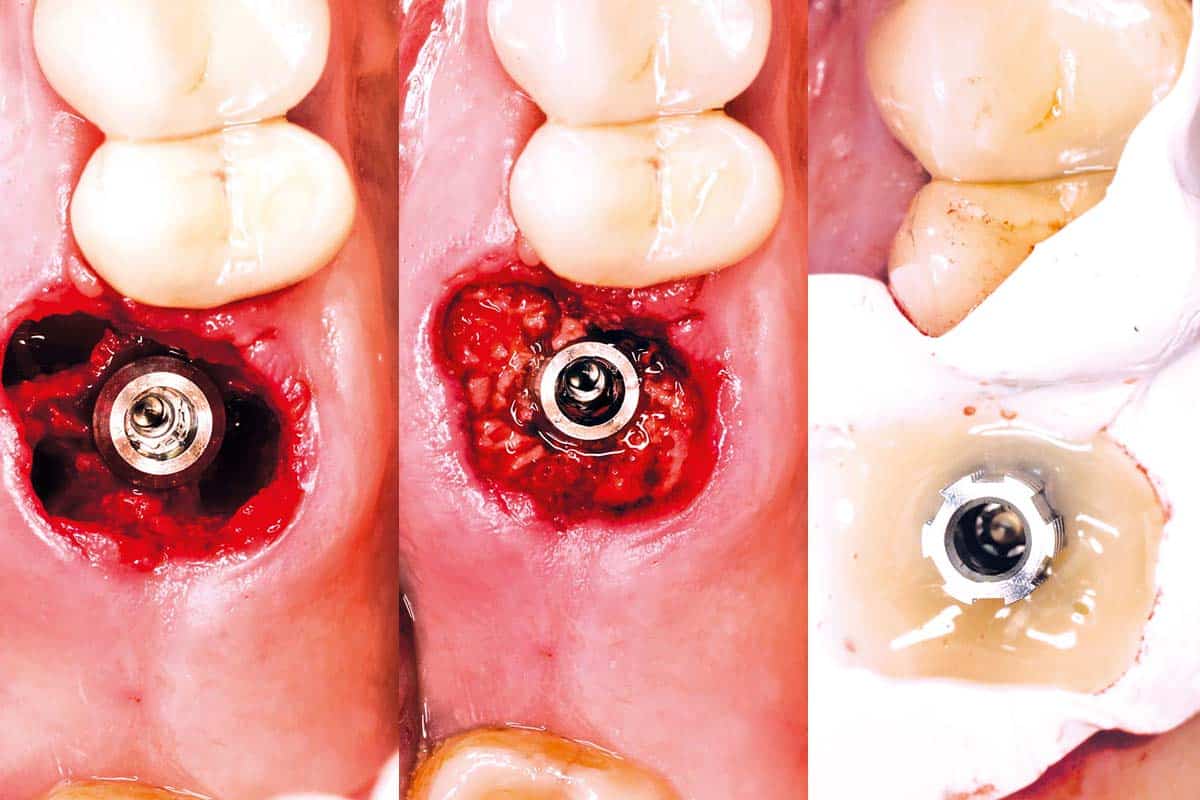
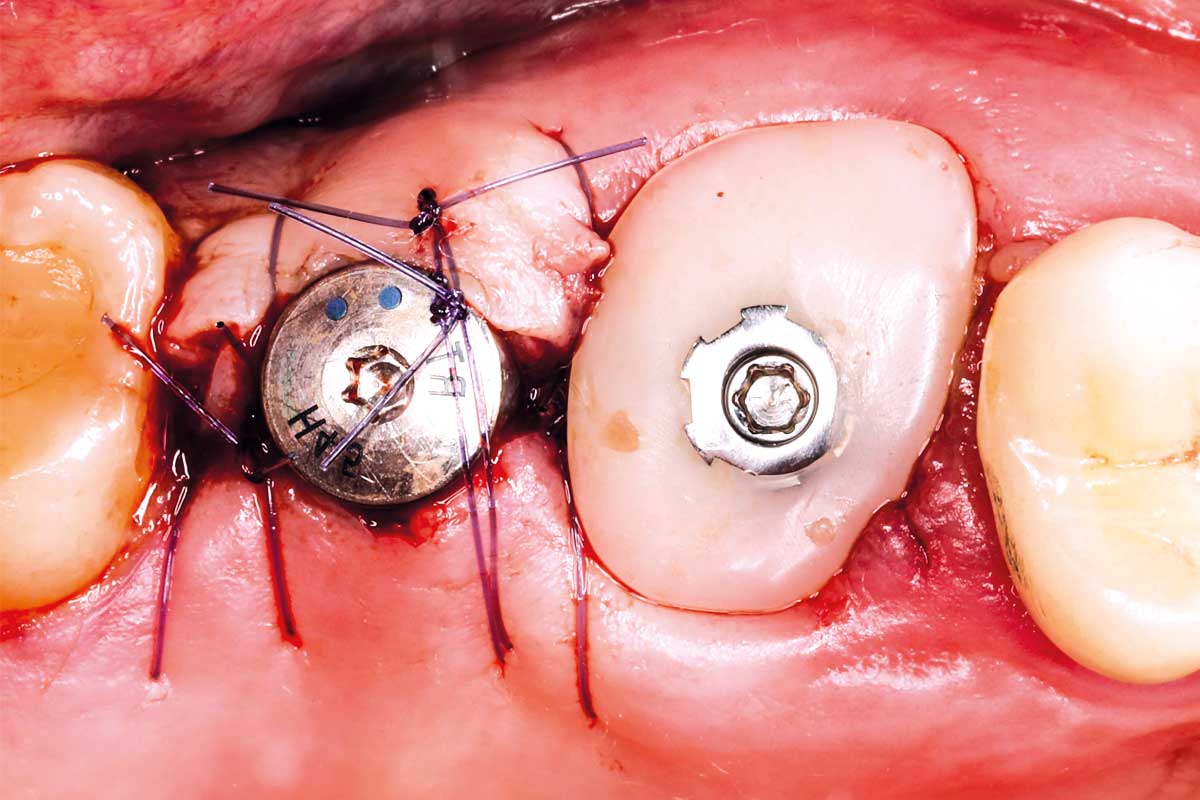
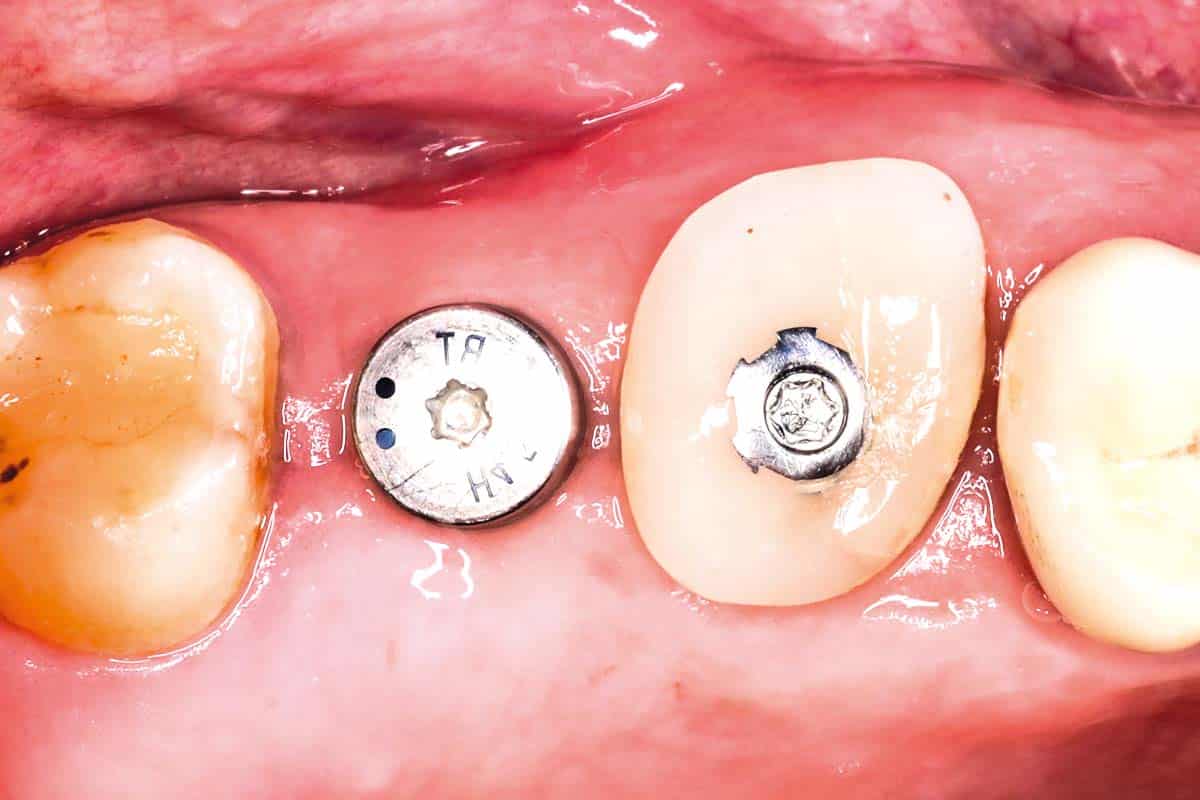
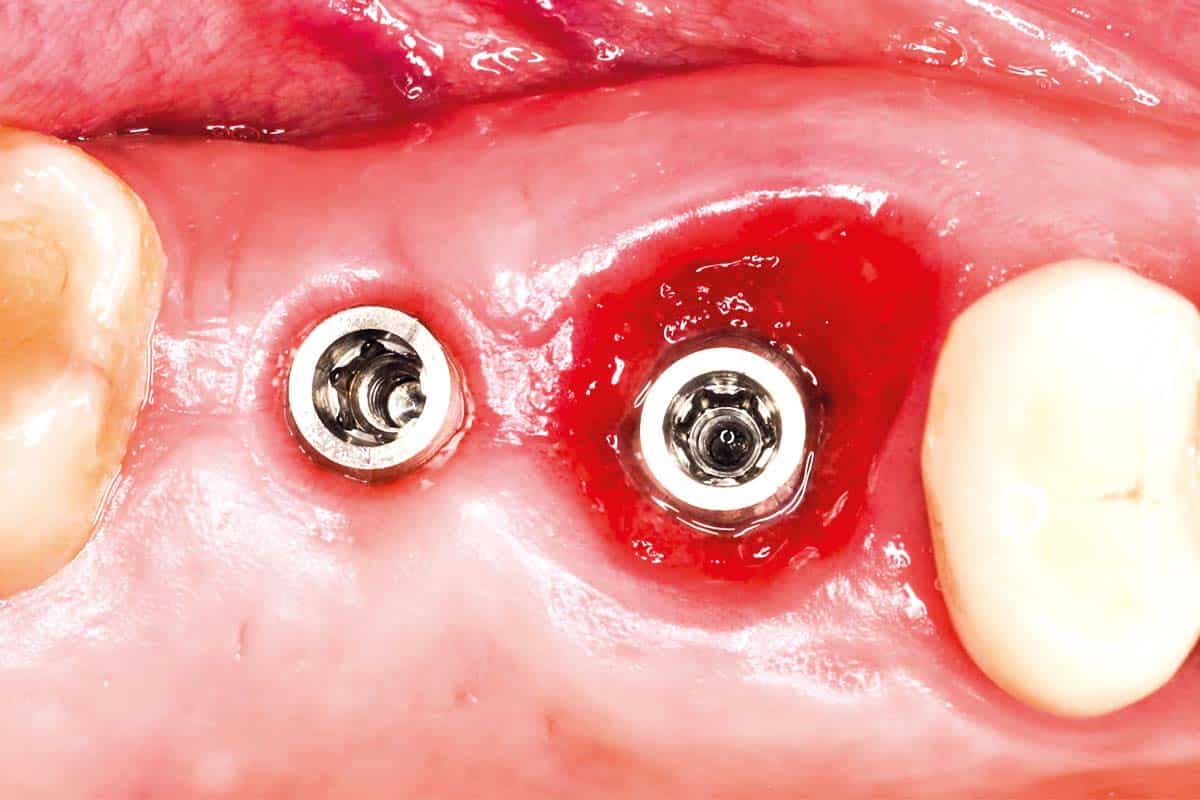
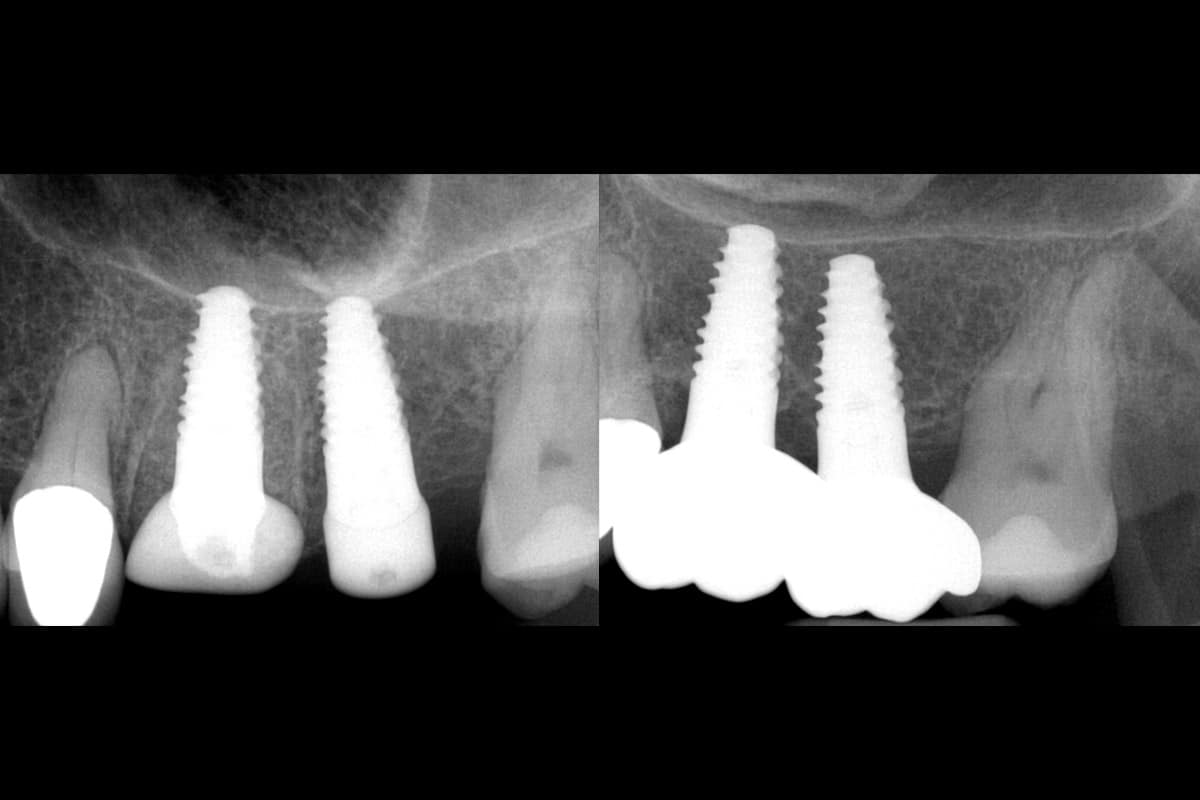
Prof. Schiegnitz: Figures 1 to 9 illustrate a specific case example: An immediate implant was placed in a patient with tooth 26 that was not worth preserving. The buccal gap between the implant and the bone wall was augmented with maxgraft® + HyA. Targeted hydration created a malleable, “sticky” consistency that could be easily inserted into the defect. A socket sealing abutment in combination with Teflon tape stabilized the material and enabled tension-free coverage. Soft tissue healing was uneventful, and radiological follow-up showed a stable peri-implant bone structure with complete preservation of the buccal contour.
CASE STUDY 1 – Immediate implantation 26 with gap filling



What is your approach to more complex sinus floor augmentation?
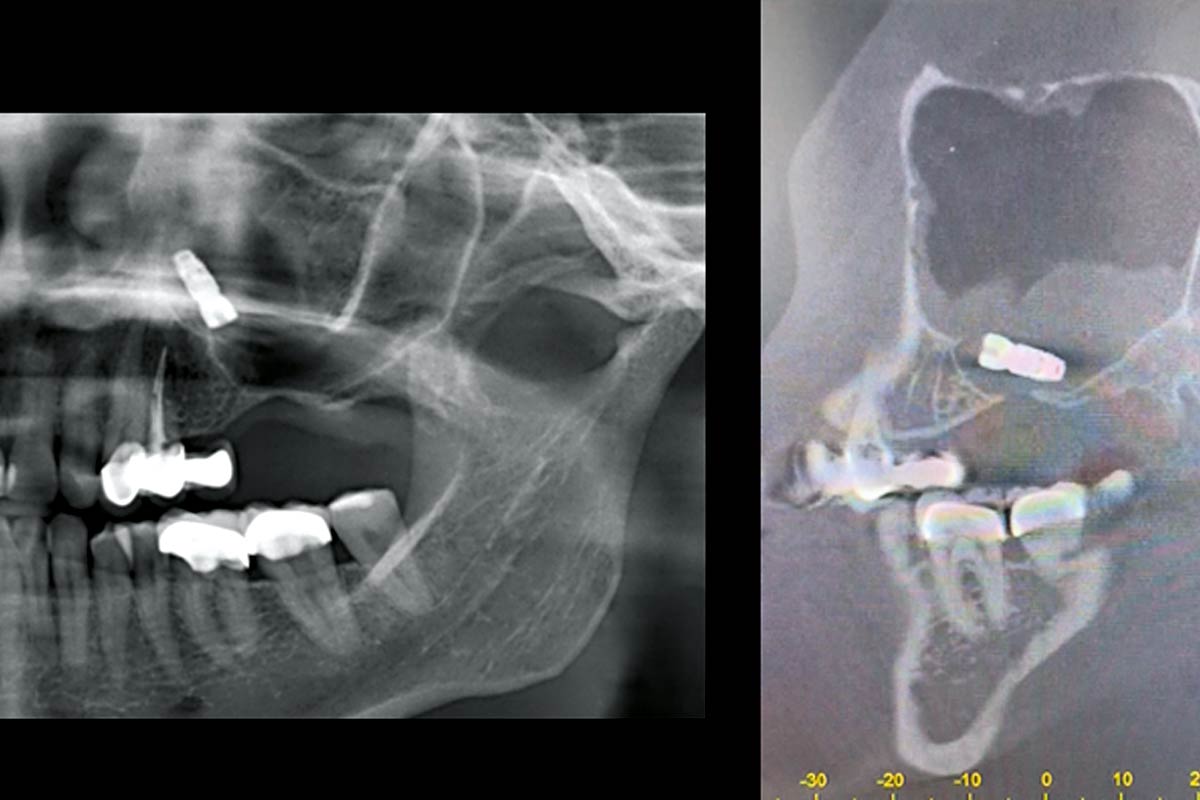
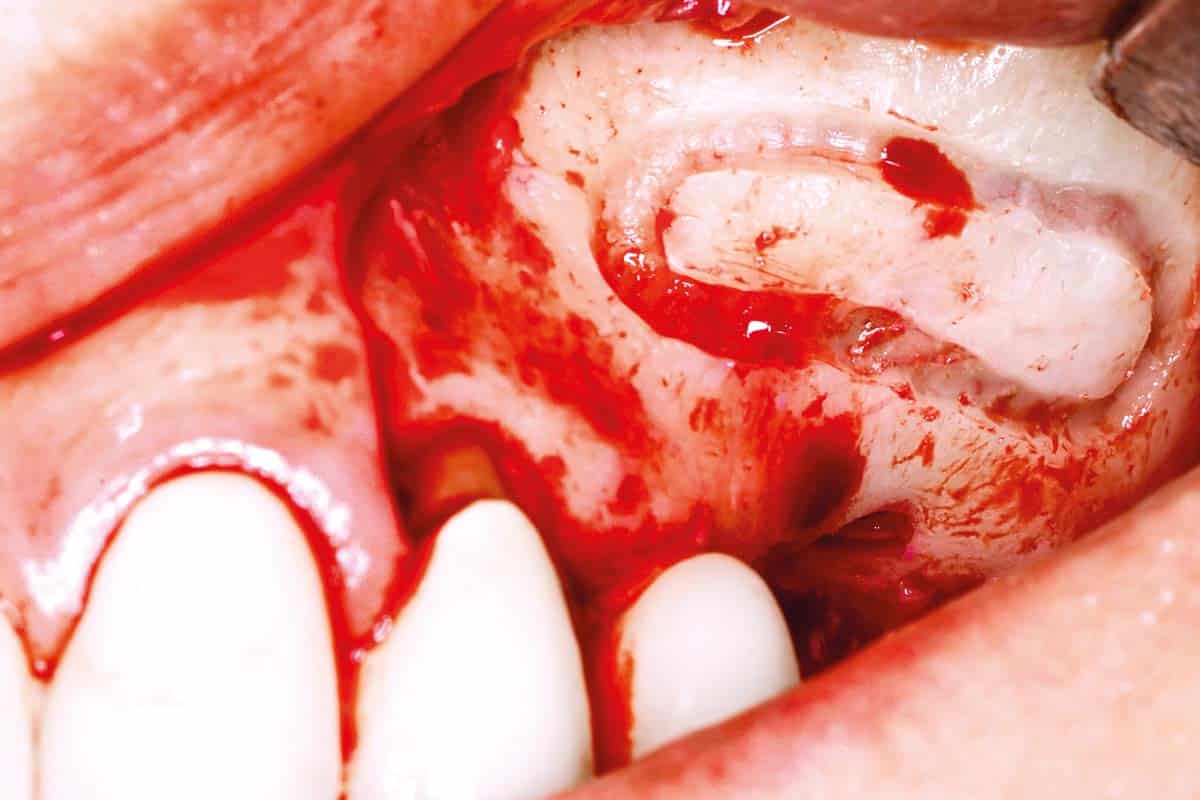
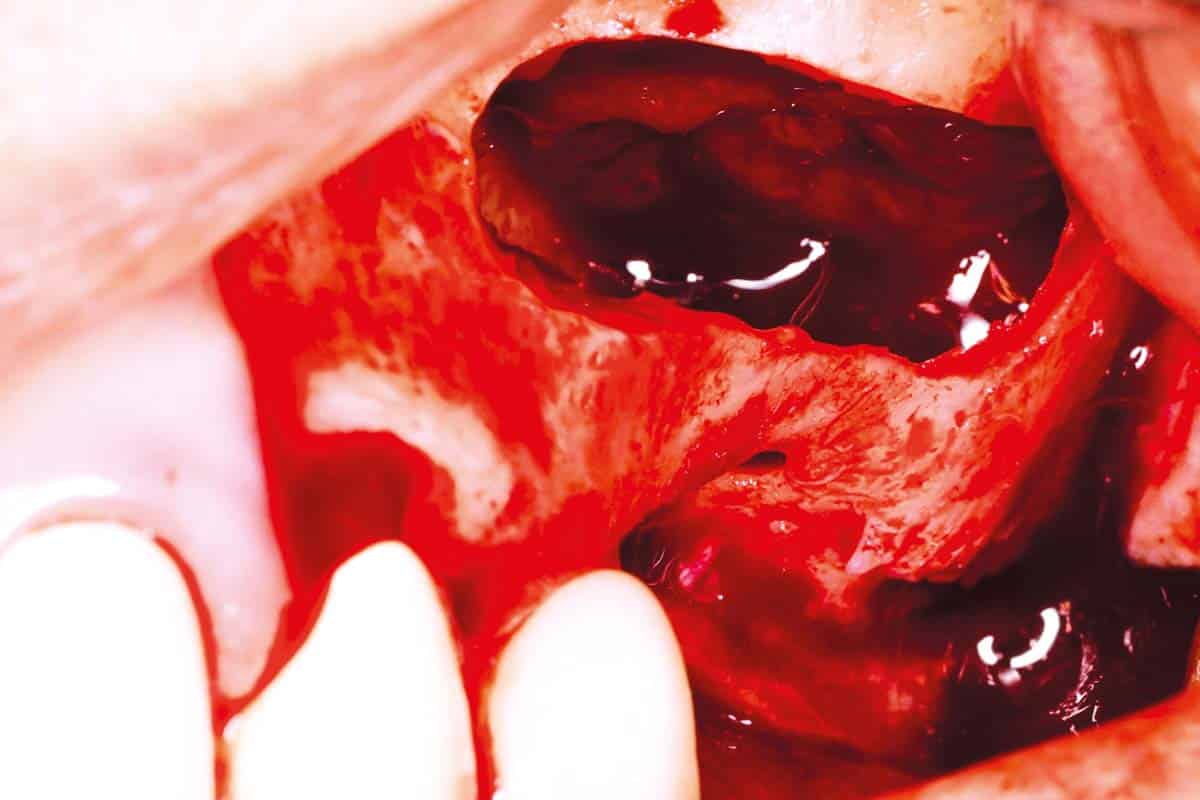
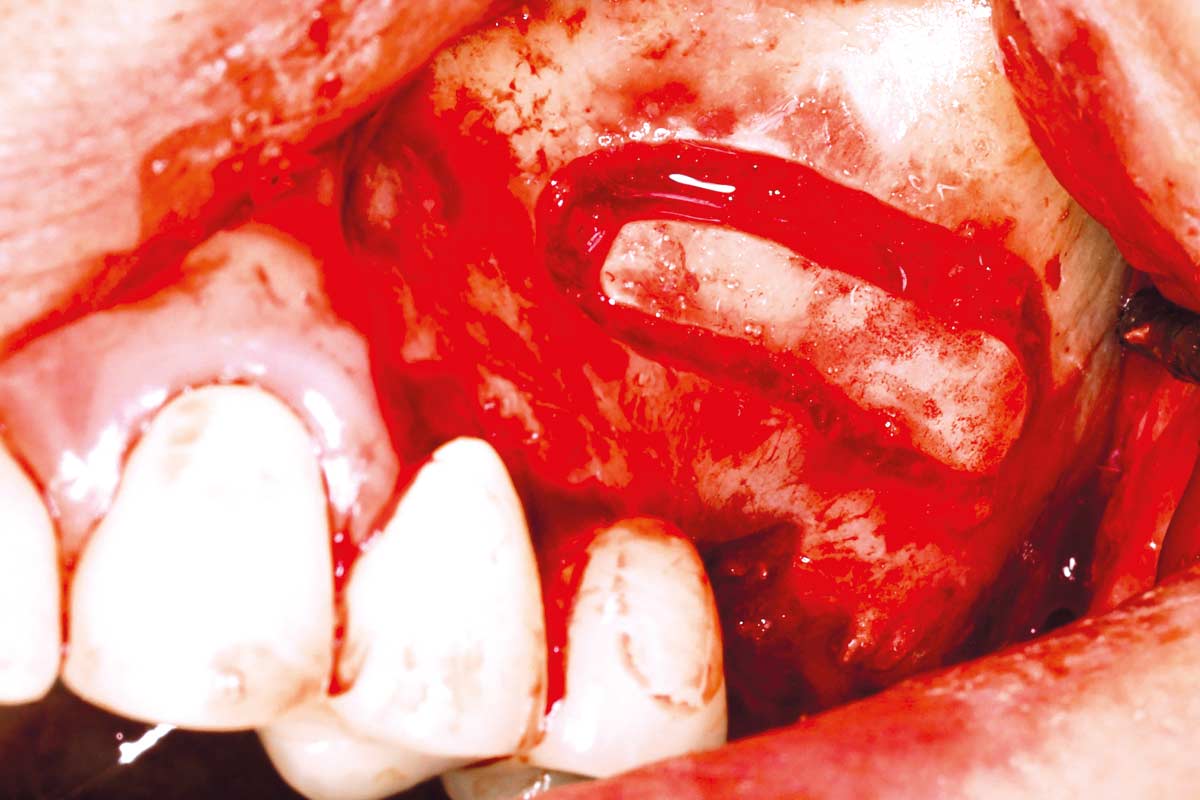
Prof. Schiegnitz: In one specific case, re-augmentation was required in region 26 after a previously inserted implant had become displaced into the left maxillary sinus. First, the lateral maxillary sinus window was prepared using piezo surgery and the displaced implant was carefully removed.
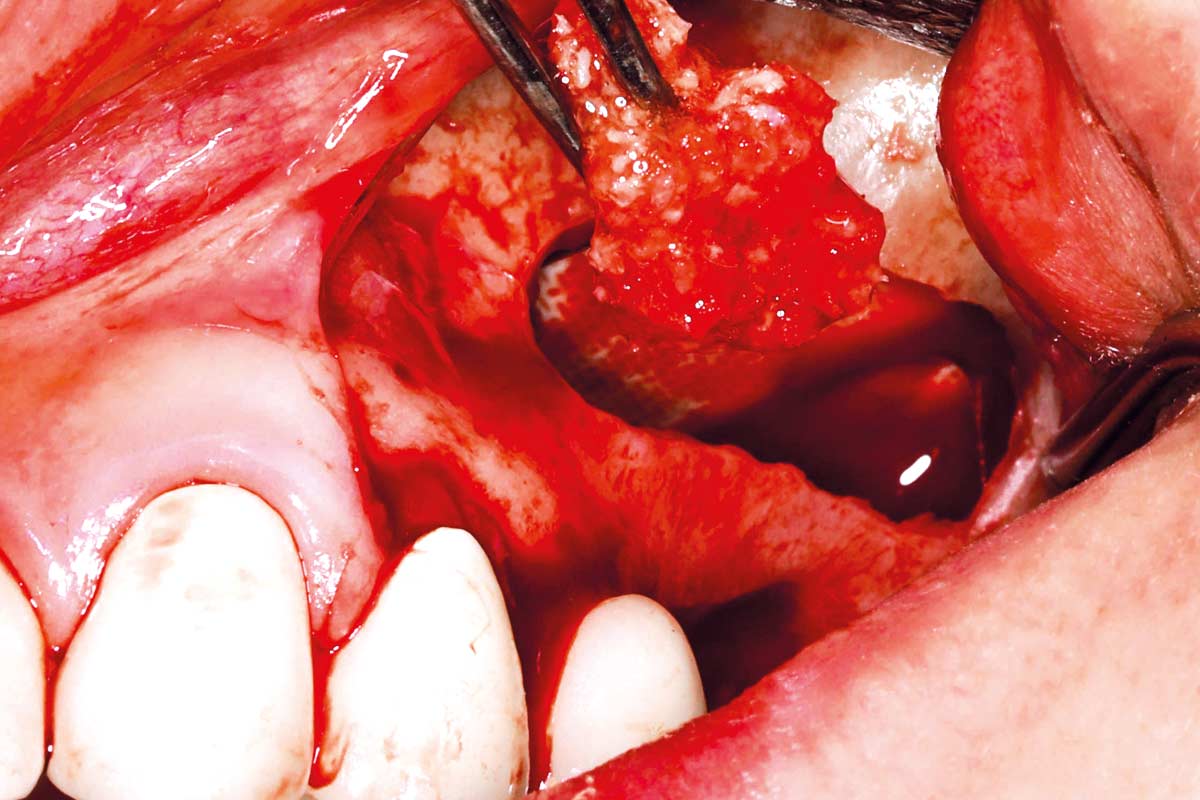
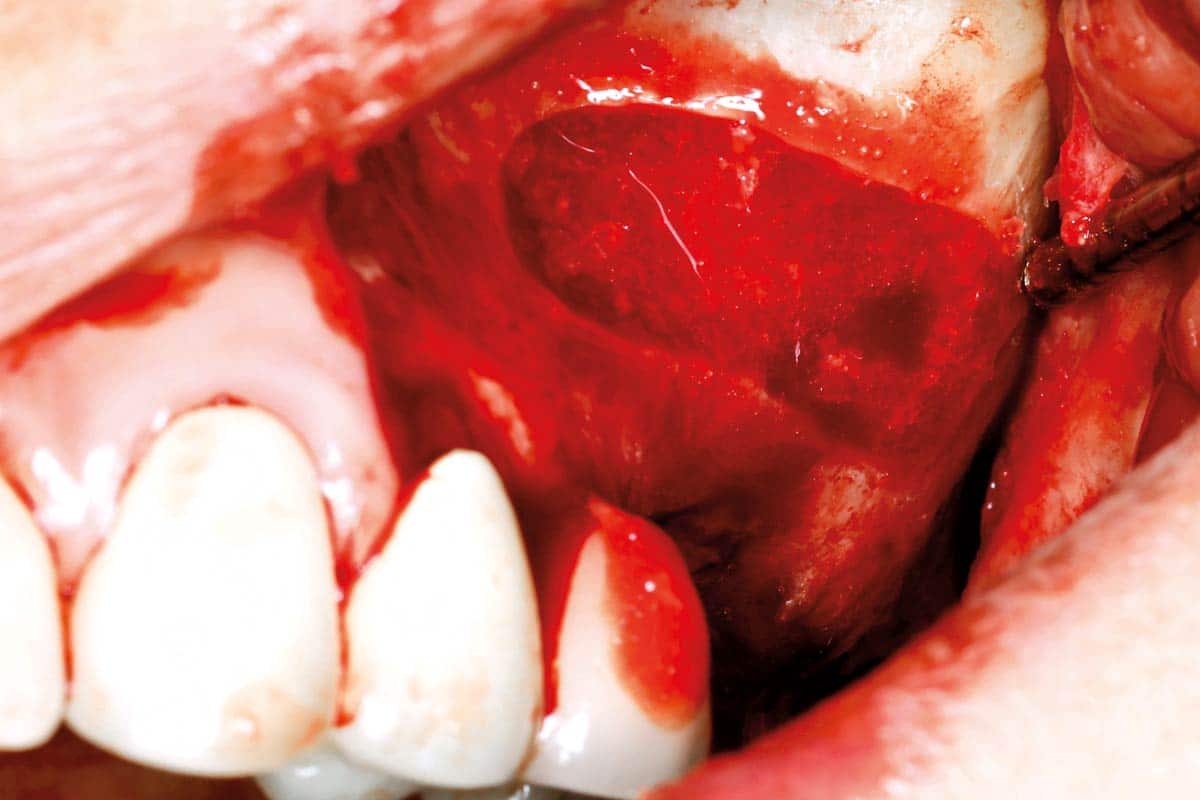
An internal sinus lift was then performed with maxgraft® + HyA with the aim of achieving volume-stable bone regeneration using a minimally invasive procedure. Thanks to its easily moldable consistency, the bone grafting material could be inserted precisely and dimensionally stable under the maxillary sinus floor.
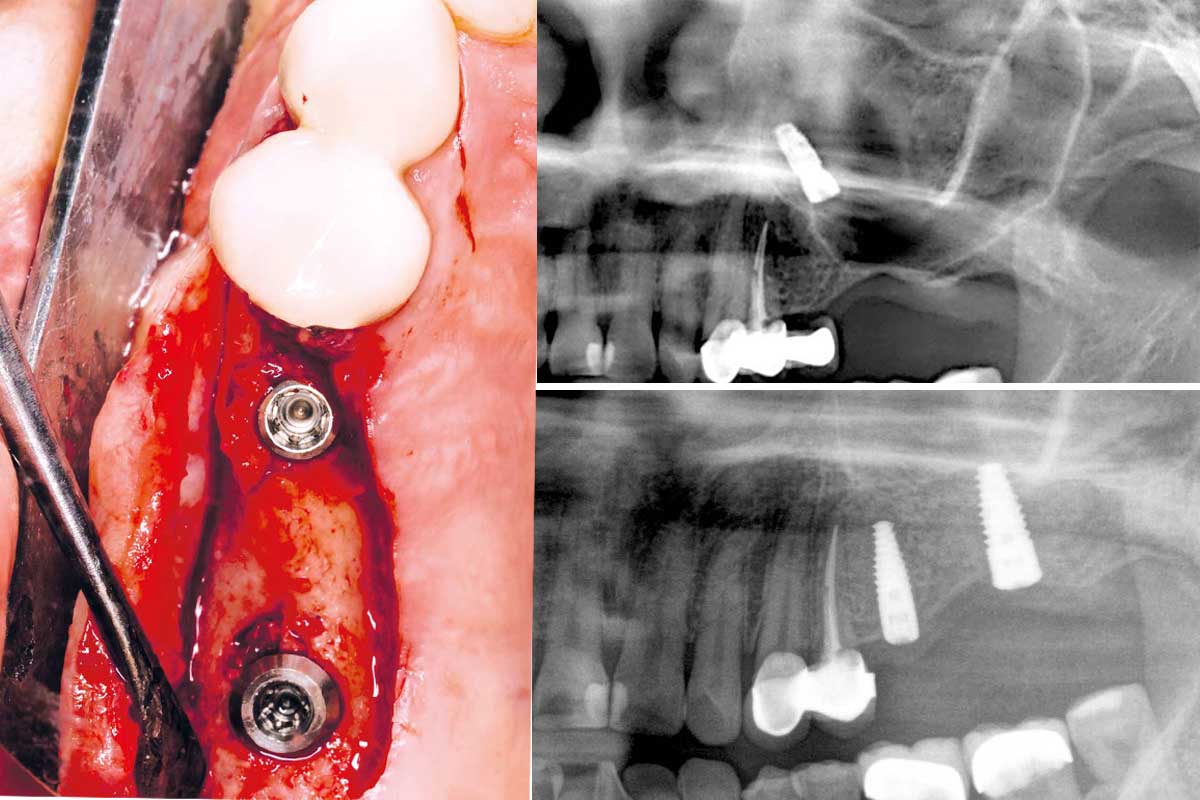
Over the course of treatment, dense, structured new bone formation and stable soft tissue conditions were observed, allowing for reimplantation without any problems.
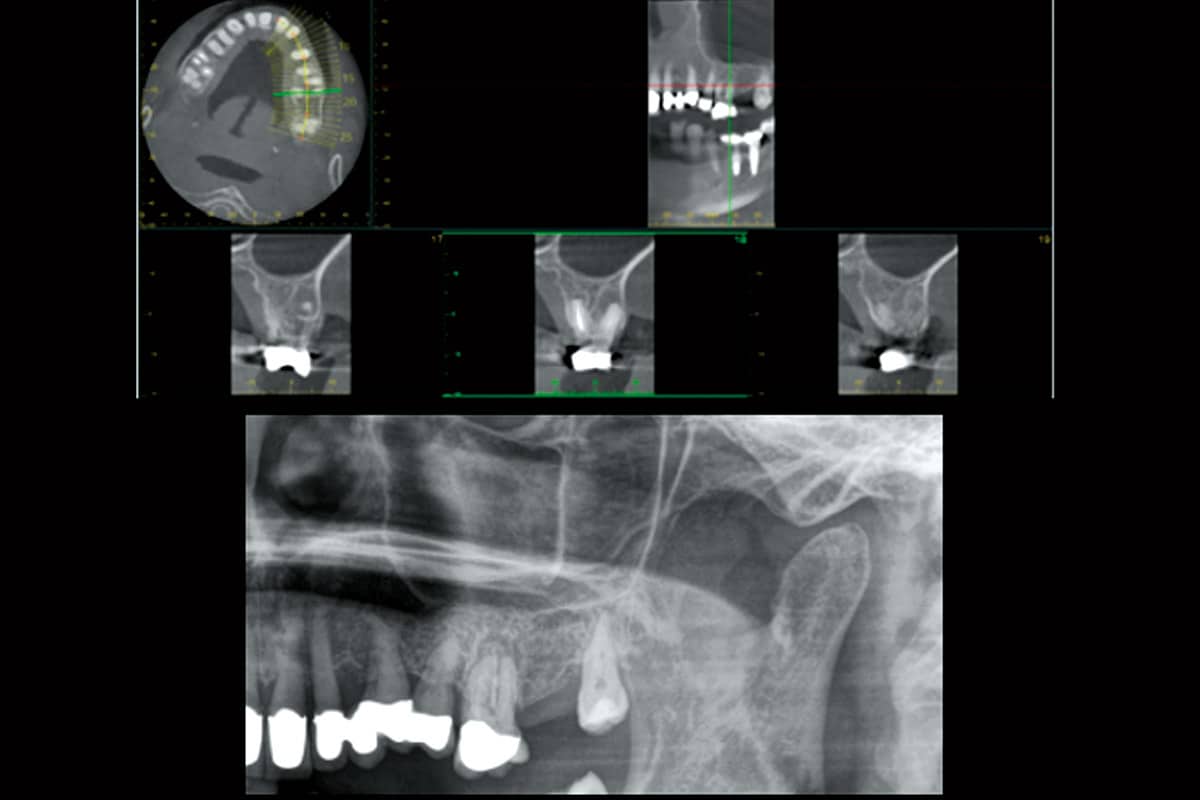
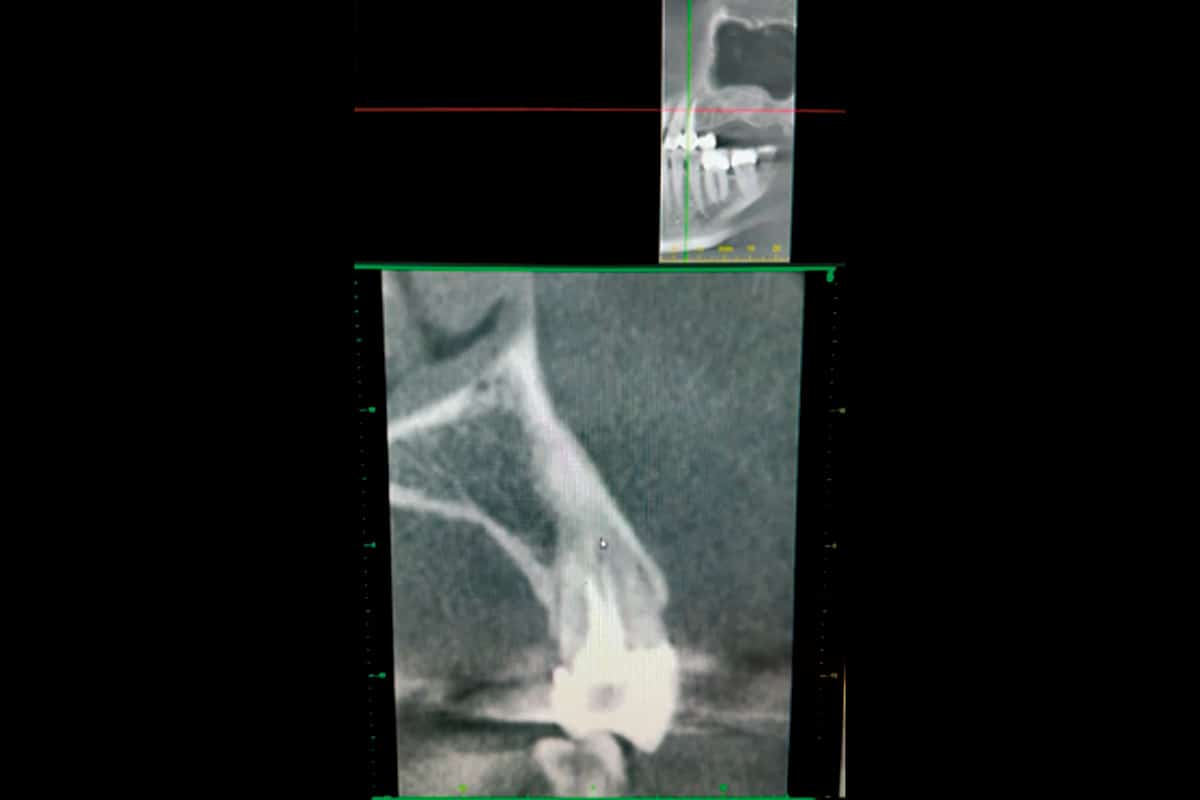
The CBCT control four months postoperatively confirmed a significant bone volume with a homogeneous structure in the augmented area. The subsequent implantation was uneventful. The volume gain and successful integration of the augmentation material were impressively demonstrated by comparing the CBCT images taken before and after augmentation. Figures 10 to 19 illustrate the course of treatment.
CASE STUDY 2 – External two-stage sinus lift with displaced implant in the left maxillary sinus area

Were there any special features or complications associated with the material?
Prof. Schiegnitz: No, on the contrary: both procedures were completely complication-free, both intraoperatively and postoperatively. During exposure, the tissue was found to be very well vascularised with stable bone integration. There were no signs of an overreaction or increased inflammation.
How would you rate the quality of bone regeneration after using maxgraft® + HyA, and are there any differences in the further clinical course compared to other augmentation materials?
Prof. Schiegnitz: Bone regeneration was extremely efficient in my cases. Volume stability proved to be excellent both horizontally and vertically. Histologically, a dense, well-vascularized bone structure was evident, and drilling stability during implant placement was also convincing which is an important criterion for the clinical load-bearing capacity of the newly formed bone.
In the further course, I observe a very harmonious integration with maxgraft® + HyA. Soft tissue healing is predictable and complication-free. During exposure, the augmented bone is often already so remodelled into patient´s own bone that hardly any post-treatment is necessary. This not only saves time in the operating room but also facilitates the planning of subsequent steps and increases therapeutic safety.
Speaking of time: How does its use affect the duration of treatment or the possibility of earlier implantation?
Prof. Schiegnitz: In cases of moderate defects, earlier implantation is certainly possible, as the tissue quality improves more quickly. Of course, this depends on the individual case, but the greater predictability in the healing phase makes it much easier to plan subsequent procedures.
How do you assess the future potential of biologically activated materials and what would you recommend to colleagues who want to work with them?
Prof. Schiegnitz: I see great potential for everyday use in implantology and surgery. Combination materials such as maxgraft® + hyaluronic acid combine biological regeneration mechanisms with surgical efficiency. Hyaluronic acid supports cell migration, angiogenesis, and early revitalization of the graft, which is crucial for high-quality bone regeneration, even in more complex defects.
Thanks to its viscous, sticky consistency, the material can be applied and shaped precisely after mixing. This is a clear advantage, especially for minimally invasive techniques and in aesthetically sensitive areas, for example. The allogenic origin eliminates the need for a second harvesting site and is also well accepted by patients who are sensitive to xenogeneic materials. At the same time, the high volume stability provides a good basis for long-term ridge preservation and may allow for earlier implantation.
My advice to colleagues: If you want to think biologically and work efficiently at the same time, you should take a close look at this class of materials.
Thank you very much for your practical explanations and assessment!
Literature:
1 Kloss et al. Int J Implant Dent. 2024 Oct 9;10(1):42.
2 Nistor et al. Diagnostics. 2025; 15(2):137.