06 Jun 2026 | LJUBLJANA
Digital planning, execution and evaluation of horizontal- and vertical bone augmentation utilizing a novel split thickness flap design
There is an increasing need from patients suffering from advanced, stage IV periodontitis with rapid disease progression for esthetic fixed dental restorations with implant placement.
The tendency for advanced inflammatory tissue breakdown in grade C is often observed in the close vicinity of deep periodontal defects due to infection and occlusal overload, especially when the buccal alveolar plate has been destroyed. Singular intrabony defects are less commonly seen in untreated cases, rather confluent pocket formation occurs.
If periodontal reconstructive therapy in advanced cases is not applicable on all involved teeth, additional targeted removal hopeless teeth with alveolar ridge preservation has to be performed simultaneously to reduce or completely avoid the need for further hard tissue reconstructions.
However, in some cases horizontal and/or vertical ridge augmentation is inevitable. Surgical techniques used today to preserve or augment deficient ridges follow biologic principles to achieve the same goal: a maintained or enlarged alveolar ridge with harmonious soft tissue contours at edentulous sites. Unfortunately, there is no consensus in literature unifying periodontal- and implant related surgical concepts.
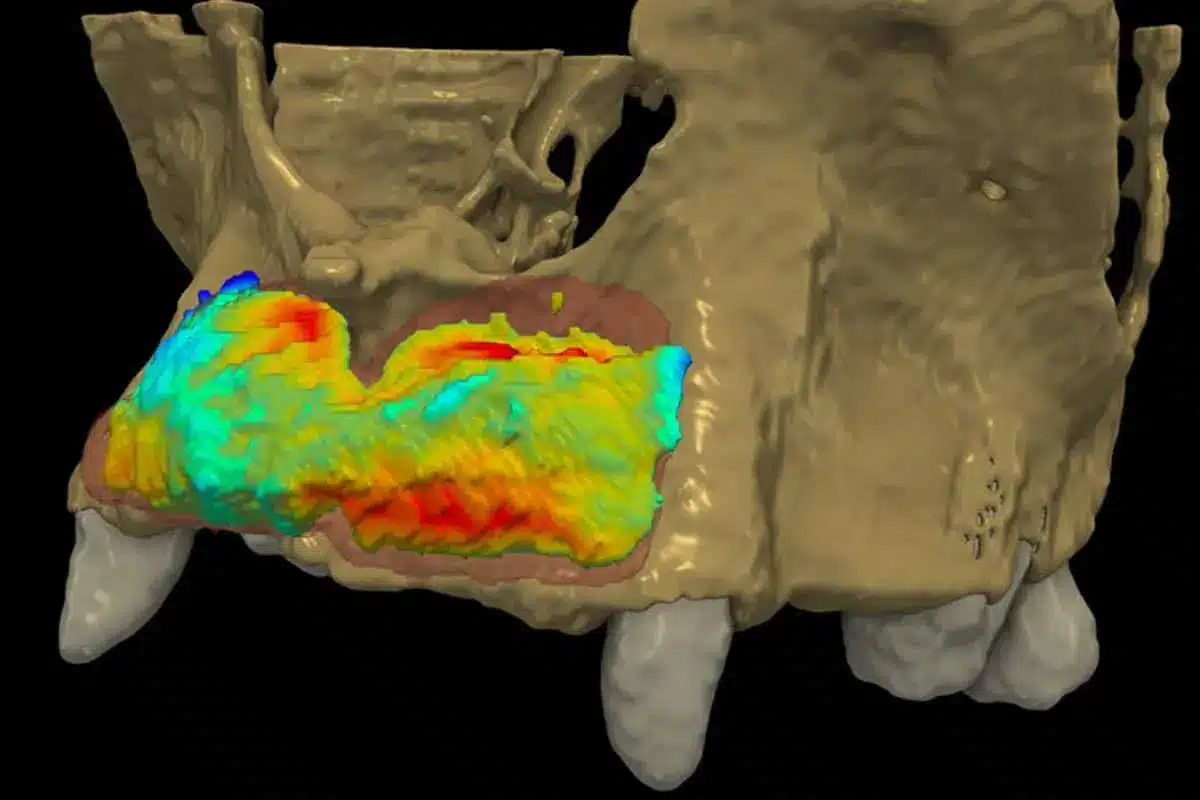
A stepwise surgical protocol has to be implemented therefore, utilizing flap designs for simultaneous ridge augmentation, socket preservation and eventually, periodontal regeneration to achieve a functional and esthetically pleasing result. The efficacy of novel surgical protocols to eliminate periodontal defects at teeth adjacent to augmented edentulous sites is of high importance to achieve favorable soft- and hard tissue conditions and to level off periimplant hard tissues to the proximal crestal bone of adjacent teeth. Advanced periodontal and alveolar ridge defects require a more precisely executed treatment concept with the aid of digital image processing and 3D visualization, allowing for individualized treatment.