CASE REPORT
Algirdas Puisys, DDS, PhD, Viktorija Auzbikaviciute, DDS, Tomas Linkevicius DDS, PhD
This case report shows successful implant placement with guided bone regeneration, simultaneous soft tissue thickening and submerged 2 mm healing abutment which we tend to call “decompression technique”. A particular technique was used in order to gain stable native bone around implant, prevent compression around implant neck and obtain proper space for the following prosthetic treatment with adequate emergence profile.
Initial situation
A 42- year old patient was referred from a colleague for the lateral ridge augmentation in the posterior mandible and simultaneous #36 implant placement. No medical history, oral or systemic health problems were mentioned which might have an impact for the treatment and following healing.
Treatment plan
During the first appointment computed tomograpghy (CT) and intraoral evaluation were performed (Fig. 1). CT revealed sufficient vertical height in the III quarter (site #36) while the horizontal bone width was insufficient for implant placement (class IV according to Cawood and Howell classification) (Fig. 2). It was decided to perform guided bone regeneration (GBR) together with 2 mm healing abutment and simultaneous soft tissue thickening.


Surgical procedure
I stage
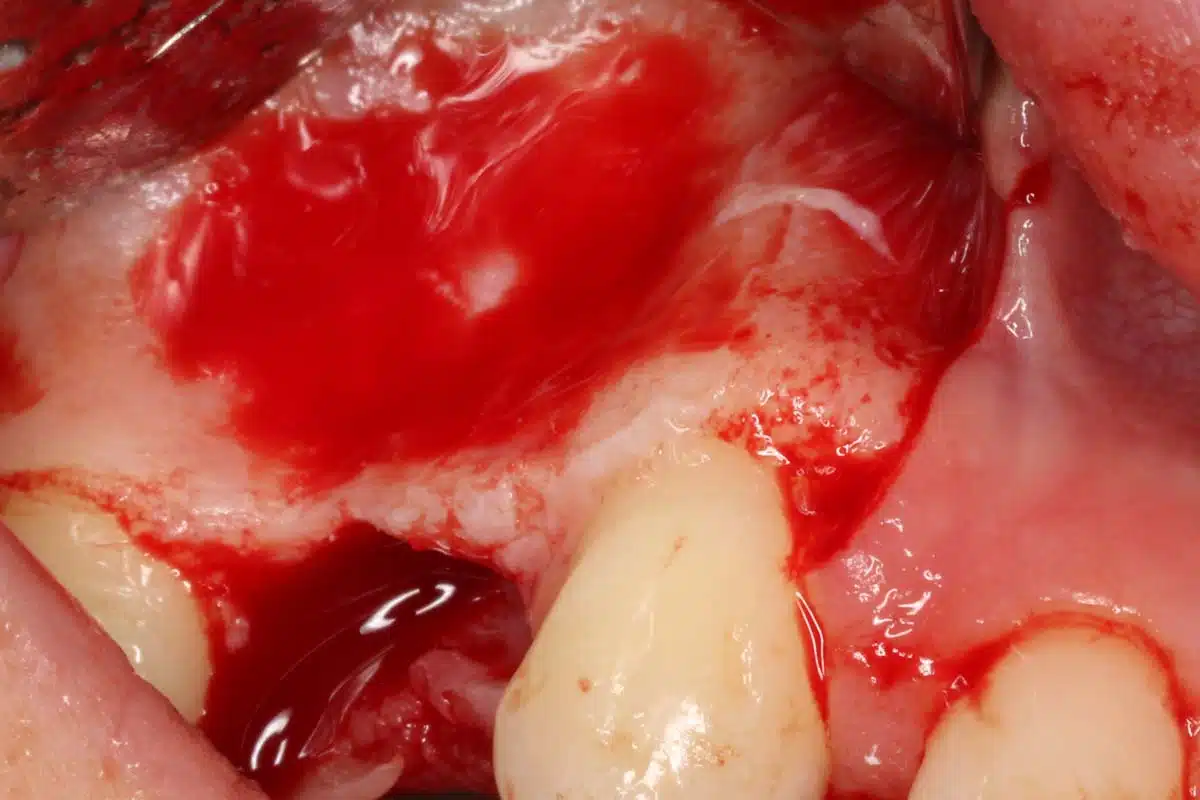
Under infiltrative local anesthesia horizontal and two vertical mucoperiosteal incisions were made to elevate the full thickness flap. Periosteum was splited with a tip of surgical scalpel blade in mucogingival junction area to obtain tension-free closure.
Buccal cortical bone was cleaned and inner side perforations were performed to increase angiogenesis for the rate of graft incorporation. Autologous bone granules were collected from the donor site of the mandible body and ramus with a cortical bone collector (Micross, META, Reggio Emilia, Italy). Subsequently, A Straumann® Bone Level Tapered Implant SLActive 4,1 x 10 mm was placed in the site #36 and good primary stability was achieved. It was decided to use 2 mm healing abutment in conjunction with submerged approach (Figs. 3-5).
A collagen tissue matrix derivate membrane (mucoderm®, botiss biomaterials, Germany) 15-20 mm in size was fitted to the defect and fixed with 3 botiss titanium pins (3 mm) at the buccal side.
Collected autologous chips were mixed with allogenic bone granules (maxgraft®, botiss biomaterials, Germany) in ratio 1:1 (Fig. 6). Patient’s blood was collected with a sterile syringe from an operating site and mixed with bone granules in order to create a stable bone mass.
Prepared bone mass was placed at the defect side; mucoderm® surrounded the bone and the ridge of the operating site (Fig. 7).
Soft tissues were sutured with 6/0 polypropilene and 4/0 cytoplast by using double simple suture technique (Fig. 8,9).
After the surgery patient received prescribed medications. In addition, she was informed about personal care requirements and importance of individual hygiene.
Sutures were removed 2 weeks after.







II stage
3 months after the last surgery patient came for second surgery to increase peri-implant soft tissue (Figs. 10,11). Fixed keratinized mucosa is mandatory factor for following prosthetic treatment and stable long-term results.
During the visit computed tomography was performed; it reveals favourable outcome of the surgery with the new bone integration (Fig. 12, 13).
Under infiltrative anesthesia connective tissue graft was taken from tuberosity donor site (Figs. 14-16). Partial-thickness flap was elevated in the site of mucogingival junction. Graft sutured with 6/o polypropylene (Fig. 17).








III stage
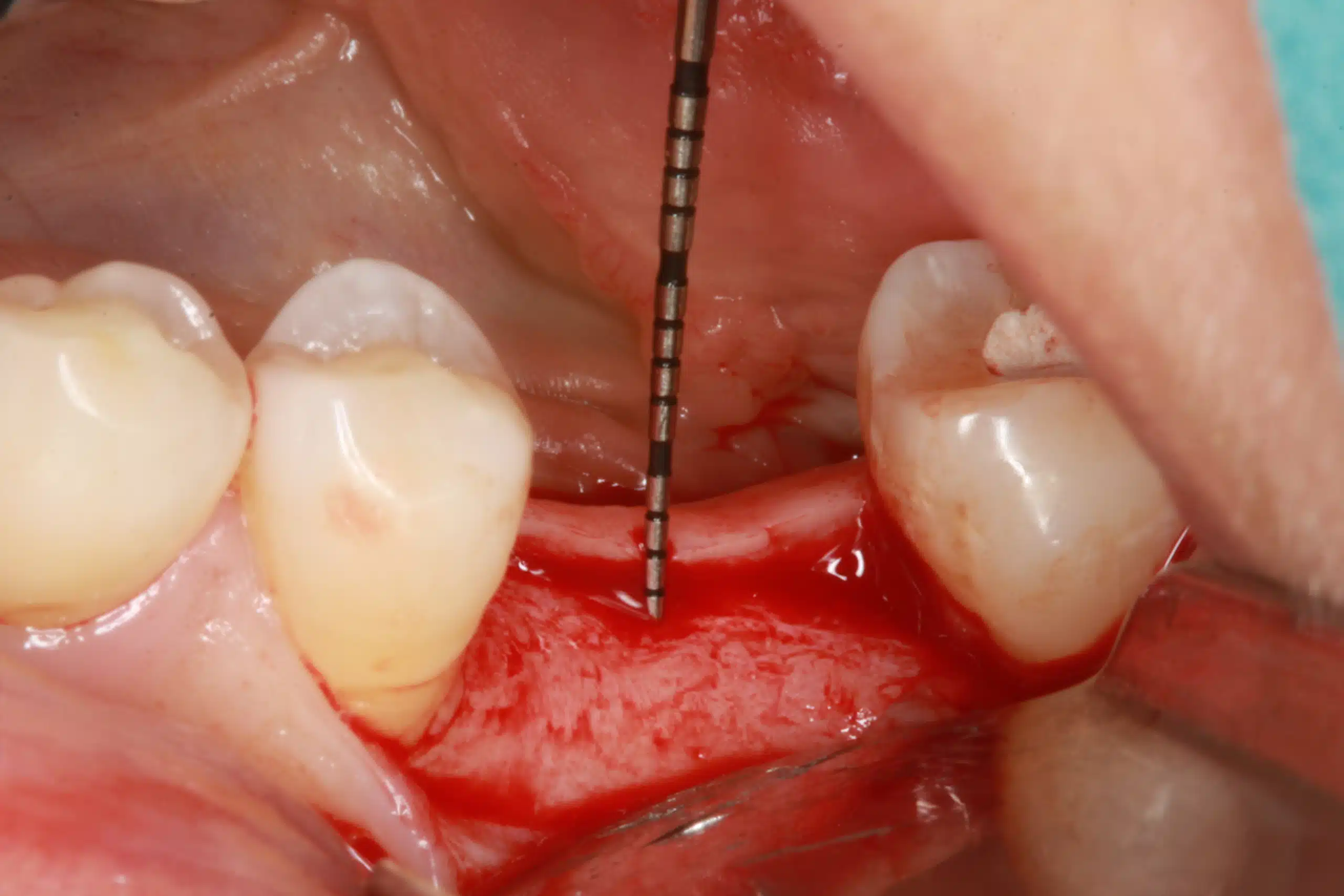
During the III stage of surgery for placing healing abutment (Fig. 18), keratinized soft tissue were analyzed and measured with periodontal probe (Figs. 19 – 26). Favourable results of bone formation around the implant neck were achieved using 2 mm healing abutment together with submerged flap technique.









Prosthetic part
3 months later after the last surgery (III stage) patient came for prosthetic treatment. Full contour zirconia crown was placed on implant. Periapical radiographs and digital photographs reveal appropriate emergence profile with stable keratinized tissue around the crown (Figs. 27 – 30).




Also interesting
- Dr. Algirdas PuišysLithuania