Study
https://doi.org/10.3390/ma15030733
Steigmann L, Di Gianfilippo R, Steigmann M, Wang HL. Materials (Basel). 2022 Jan 19;15(3):733.
BACKGROUND AND OBJECTIVE
Tooth removal inevitably results in dimensional reductions of the alveolar process. Alveolar socket and ridge preservation procedures have been demonstrated to minimize ridge resorption after tooth extraction. However, although the present clinical literature suggests different treatment modalities for ridge preservation, a guideline on when to use which kind of grafting material is currently missing. Therefore, the aim of this study was to provide decision guidance for the most suitable ridge preservation technique.
APPROACH
The authors performed a systematic literature search to define parameters with respect to the phenotype of alveolar sockets that affect the outcome of ridge preservation procedures. Buccal bone thickness, buccal bone integrity, and dehiscences or fenestrations of the buccal bone wall were found to be crucial factors. Thus, based on the morphology of the labial bone wall a classification of extraction sites and a treatment decision tree was proposed.
CLASSIFICATION OF EXTRACTION SOCKETS
Based on the buccal bone characteristics, three types of extraction sockets were described:
- Socket type 1 (ST1): sockets with intact buccal bone wall
- Socket type 2 (ST2): sockets with buccal bone fenestration
- Socket type 3 (ST3): sockets with buccal bone dehiscences that affect bone height
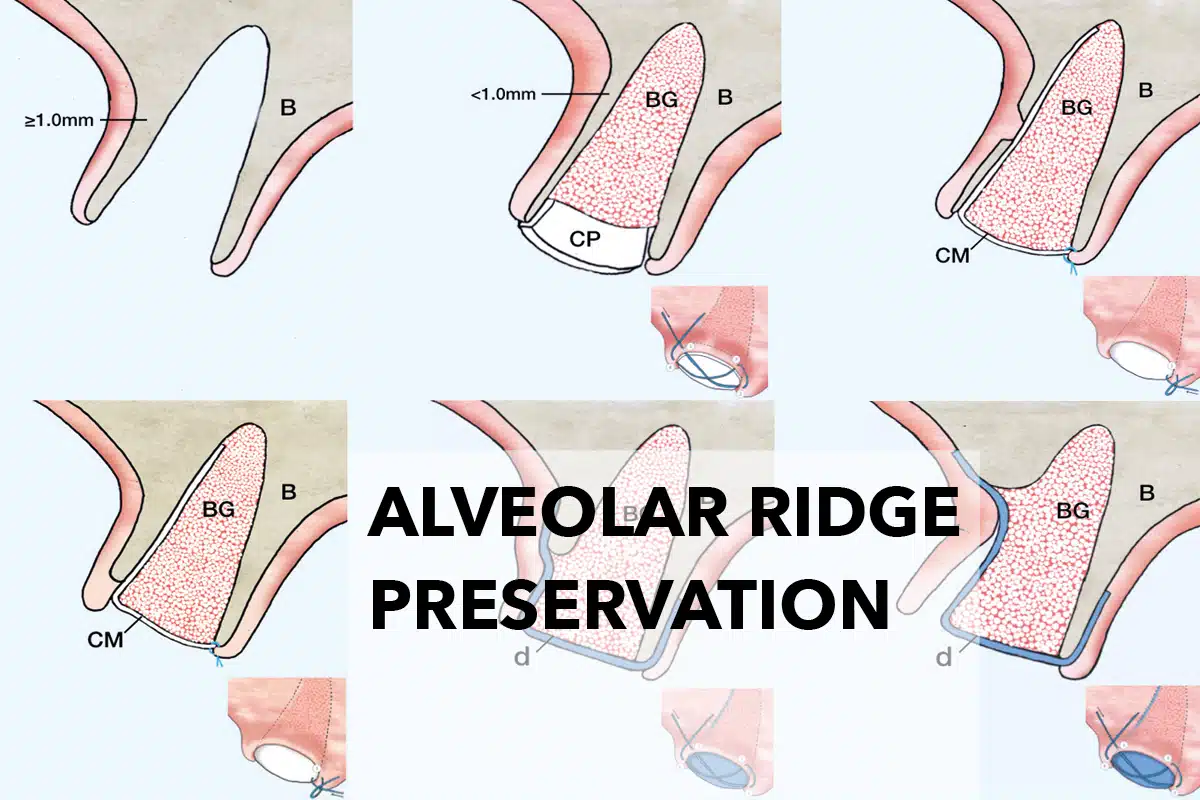
Sockets type 1 are additionally subdivided based on the thickness of the bone wall, i.e. ≥ 1.0 mm (subclass ST1A) or < 1.0 mm (subclass ST1B) thickness. Similarly, sockets type 3 are further divided according to the dehiscence height, i.e. 1/3 (subclass ST3A), 1/3 – 2/3 (subclass ST3B) or ≥ 2/3 (subclass ST3C) of the buccal bone height.
PROPOSED TREATMENT OPTIONS
Based on the defined types of extraction sockets different treatment modalities were proposed.

Fig. 1. Proposed biomaterials and treatment approaches for the different socket types.
Socket type 1 (ST1) – Intact buccal bone wall
- ST1A sockets (thick buccal wall) generally require no treatment. However, blood clot stabilization can be supported by applying a collagen sponge.
- ST1B sockets (thin buccal wall) are filled with a particulate allograft or xenograft 1–2 mm below the alveolar crest, which is covered either by a collagen sponge or by an autogenous soft tissue graft especially in the aesthetic zone.

Socket type 2 (ST2) – Buccal fenestration
Sockets with a fenestration defect at the labial bone wall can be treated with a particular grafting material and a collagen membrane applied according to the ice-cream-cone technique, which omits the need of flap reflection.

Socket type 3 (ST3) – Buccal bone dehiscence
Treatment approaches for sockets presenting with a dehiscent buccal bone wall are based on the use of a particulate bone substitute in conjunction with a barrier membrane.
- Sockets with a dehiscence of less than one third of the buccal bone height (ST3A) can be treated using the same approach as for the treatment of type 2 sockets.

- If the dehiscence is between one third and two thirds of the buccal bone height (ST3B) a tunnel approach is proposed. After detachment of the periosteum from the bone using a tunneling instrument, the socket is filled with the bone grafting material. A dense PTFE membrane is tugged into the created space to cover the graft and at least 3 mm of native bone on the buccal and the oral side. The membrane is fixated by sutures and left exposed to the oral cavity.

- Sockets with a dehiscence extending two thirds of the buccal bone height (ST3C) are approached by flap reflection both on the labial and oral side. The use of a dense PTFE membrane allows for open healing and thus the maintenance of the soft tissue architecture.

CONCLUSION
The anatomical structure of the buccal bone plate guides the treatment approach and biomaterial selection for the different socket types.
BIOMATERIAL RECOMMENDATIONS
– collacone® for sockets with intact, thick bone wall (Type 1A) to support the blood clot
– For thin, dehiscent or absent buccal bone (Type 1B, 2 and 3), cerabone® (bovine), maxgraft® (allograft) or maxresorb® (synthetic) are options for grafting
– mucoderm® for sockets with intact, thin bone wall (Type 1B) to seal the site and to protect the grafting material
- Clinical Case by Dr. Massimo Frosecchi (mucoderm® alone)
- Clinical Case by Dr. Massimo Frosecchi (in combination with maxresorb®)
- Clinical Case by Dr. Algirdas Puišys (in combination with maxgraft®)
– collprotect® membrane for Ice Cream Cone Approach (Type 2 and 3A sockets)
- Type 2https://botiss.com/product/classification-based-on-extraction-socket-buccal-bone-morphology-and-related-treatment-decision-tree/
- Type 3A – Surgery by Dr. Alfonso Caiazzo (in combination with maxresorb®)
– permamem® for severely dehiscent sockets
Also interesting
- RECORDED-WEBINAR




 Dr. Dragana RakasevicSerbiaDr. Miguel StanleyPortugalProf. Anton SculeanSwitzerlandDr. Marius SteigmannGermany
Dr. Dragana RakasevicSerbiaDr. Miguel StanleyPortugalProf. Anton SculeanSwitzerlandDr. Marius SteigmannGermany - Study